
Accessible Healthcare
Health and illness are with us for the whole span of our life. We have been fighting diseases since the day we were born. We work, we study, we eat, and we sleep. However, we cannot accomplish a single task without a properly functioning body. So, we pay to maintain our bodies healthy. We pay to various healthcare institutions: hospital, doctor’s offices, clinics, nursing homes. We pay to receive services through our healthcare system. The quality of medical service we receive is based on the quantity we pay.
Thus, leading to question the fairness of the American healthcare system. Are we segregated into different consumer groups by our purchasing power in the healthcare system? Will we suffer or die from a healable disease because we are too poor to afford treatment, yet not poor enough to qualify to acquire health insurance? If you live in the United States, the answer is Yes.
In the United States, about 700,000 people go bankrupt due to their inability to pay medical bills. In comparison, France, Japan, Germany, the Netherlands, and Canada have 0 bankruptcy cases in the same field. Thus, it is not unreasonable to claim that the U.S. has the most unaffordable health care system compared to other developed countries where the cost is complementary to its services. A direct reason for this issue consists of the complexity of the U.S. Healthcare system.
The healthcare system was first implemented in the social system and sprouted all over the world from Europe to the U.S. in the early 1900s. It is used as a way to connect patients to different nodes in various health care institutions and personnel. Specifically to the US, the healthcare system (labeled as "exceptionalism") resembles a hotpot of a mixture of 4 types of health care models: Bismarck, Beveridge, National Health Insurance and Out-of-pocket Model, corresponding to different age sectors and social groups. The table below attempts to depict the complexity of the American Health model.

Different systems constitute one healthcare structure; however, the models cannot fully illustrate the complexity of the U.S. system. One paramount distinction the U.S. healthcare system is its for-profit nature. Rather than a health care system, it mirrors more a business system. All the profits earned by the institutions go to the hands of shareholders as opposed to providing medical services to the public.
According to the graph below, since the late 1990s to 2010s, the costs of healthcare services doubled, rocketing up from around 9% in the year 1980 to 17.1% in the year 2013. By 2016, spending on healthcare contributes to 17.8% of the U.S. GDP 2.
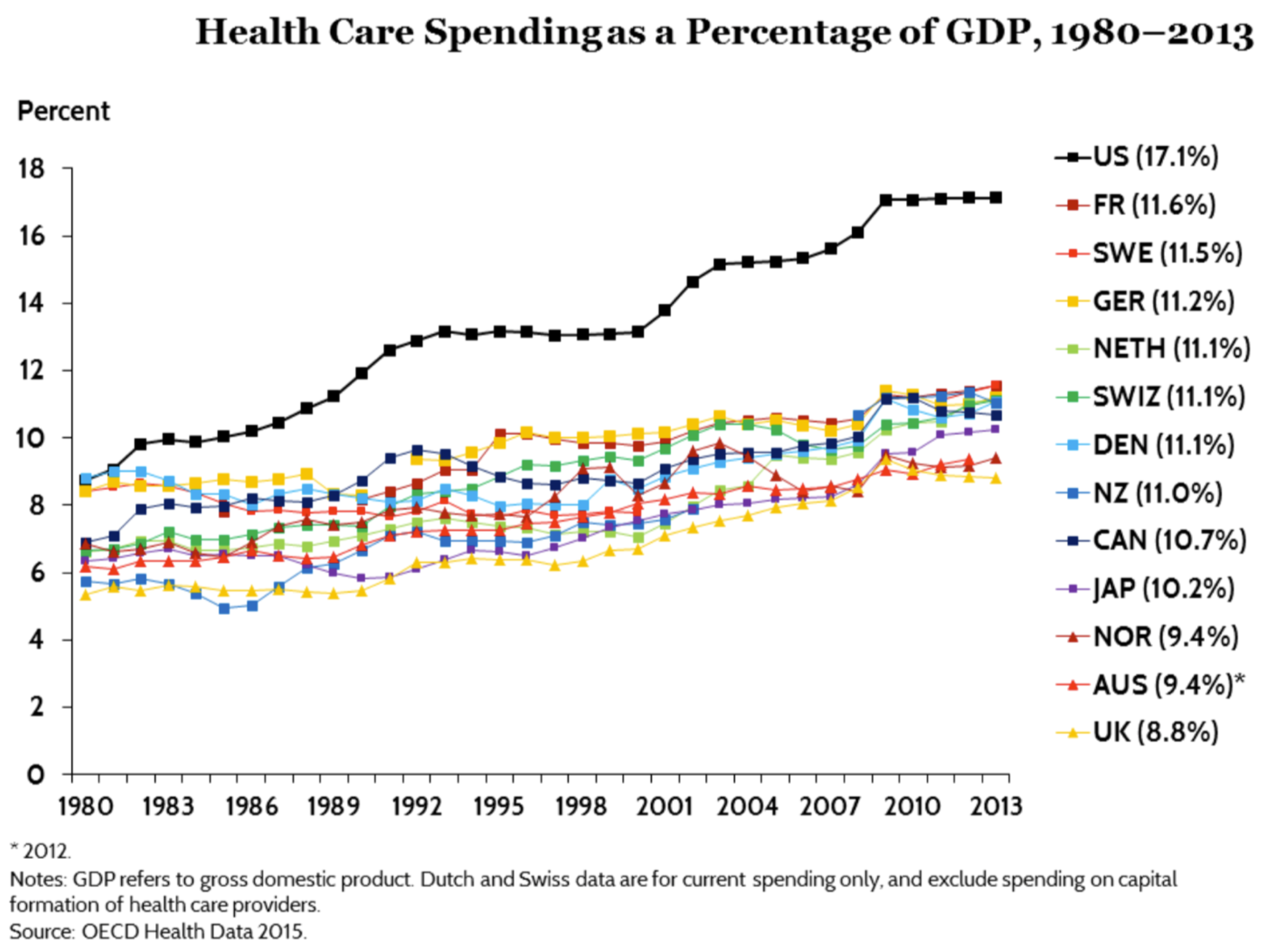
The rising trend in cost has sparked controversies. Positively, increasing spending on health care benefits the specialists who work under intense pressure and with the fast-paced schedule. Nevertheless, expensive healthcare products do not equalize the quality of the services the citizens receive. When the U.S. has only 4.0 annual physician visits per capita, Japan, which has around 7% lower spending as a percentage of GDP on health care has three times more annual physician visits (12.9 vs 4.0) per capita.

The inaccessibility of healthcare is let us questioning about the quality of health care we receive. Are we consuming our personal wellbeings or just for benefiting the private enterprise? Is health a privilege or a right in the U.S.? Since the beginning of the medical health care system in the U.S., presidents such as Roosevelt, Lincolns, Reagen, Obama attempted to reform the system, but only a few succeeded. The social and commercial forces intertwine with the complex nature of the system. This amounts to the complexity of the system. We do not know what the health care system will be like in the future, but we must keep our eyes on what we are living with, what our personal wellbeings are lying on and being aware of the risks we are taking.
Edited by Naomi Santiago and Julie Park.
Sources:
1 David Himmelstein et al., “Market Watch: Illness and Injury As Contributors to Bankruptcy,” Health Affairs Web Exclusive, February 2, 2005, pp. W5-62
2 “Health Care Spending in the United States and Other High-Income Countries.” Commonwealth Fund, www.commonwealthfund.org/publications/journal-article/2018/mar/health-care-spending-united-states-and-other-high-income.
3 “Current Health Expenditure (% of GDP).” Literacy Rate | Data, data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS.
Graphs:
Rosenthal, Elisabeth. “How the High Cost of Medical Care Is Affecting Americans.” The New York Times, The New York Times, 18 Dec. 2014, www.nytimes.com/interactive/2014/12/18/health/cost-of-health-care-poll.html.
Squires, David, and Chloe Anderson. “U.S. Health Care from a Global Perspective: Spending, Use of Services, Prices, and Health in 13 Countries.” The Commonwealth Fund, Oct. 2015